Difference in Spinal Levels on Follow-up Scan

This panel shows the baseline and follow-up scan. The L4-L5 interspace is marked by the iliac crest and the first vertebral body above the pelvis is L5 on the baseline scan. The follow-up scan does not scan the same vertebral bodies.
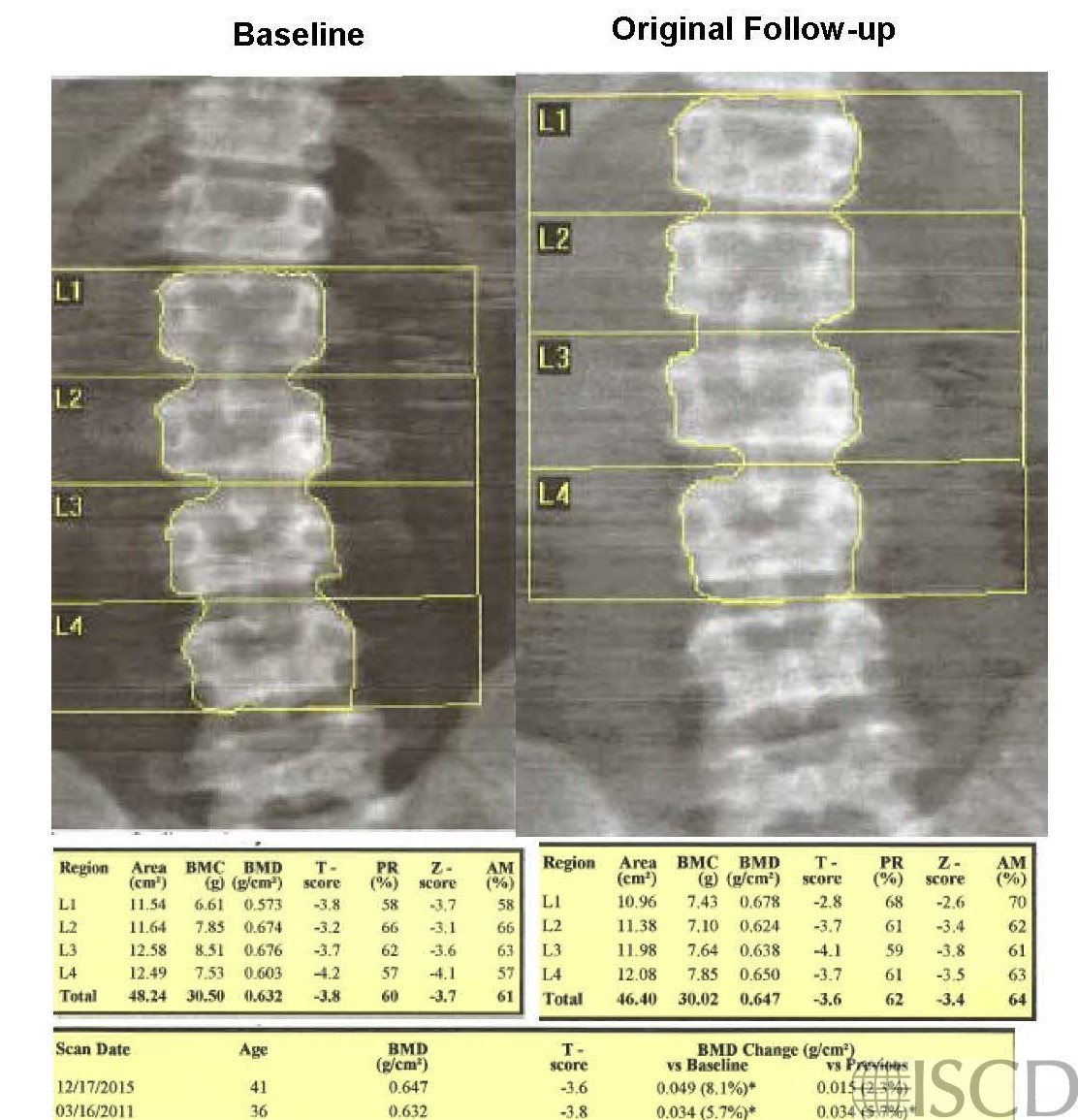
The panel shows the corrected follow-up scan. Instead of no signficant difference, there is now a significant difference using the 95% confidence intervals for the institution.

The left upper panel shows the baseline scan. Notice that there are no ribs above what is marked as L1. This scan is numbered from the bottom up. The upper right panel shows the follow-up scan. Notice that the same vertebral bodies are not scanned as in the baseline scan. The interval change that is indicated is not significant using the 95% confidence intervals for the institution. The bottom panel shows the corrected follow-up scan. There is now a significant increase using the institution’s 95% confidence intervals. For accuracy and precision, it is important to make sure the same spinal levels are always scanned.
Sarah L Morgan, MD, RD, CCD, The University of Alabama at Birmingham