DXA Interpreters Can Suspect Forearm “Slot Error” by Evaluating Tissue Thickness Measurement

Figure 1: Current and Prior Spine and Hip DXA Documenting No BMD Change

Figure 3: Current and Prior Forearm DXA (Soft tissue point-typing view) Demonstrating Differences in Soft-tissue Identification
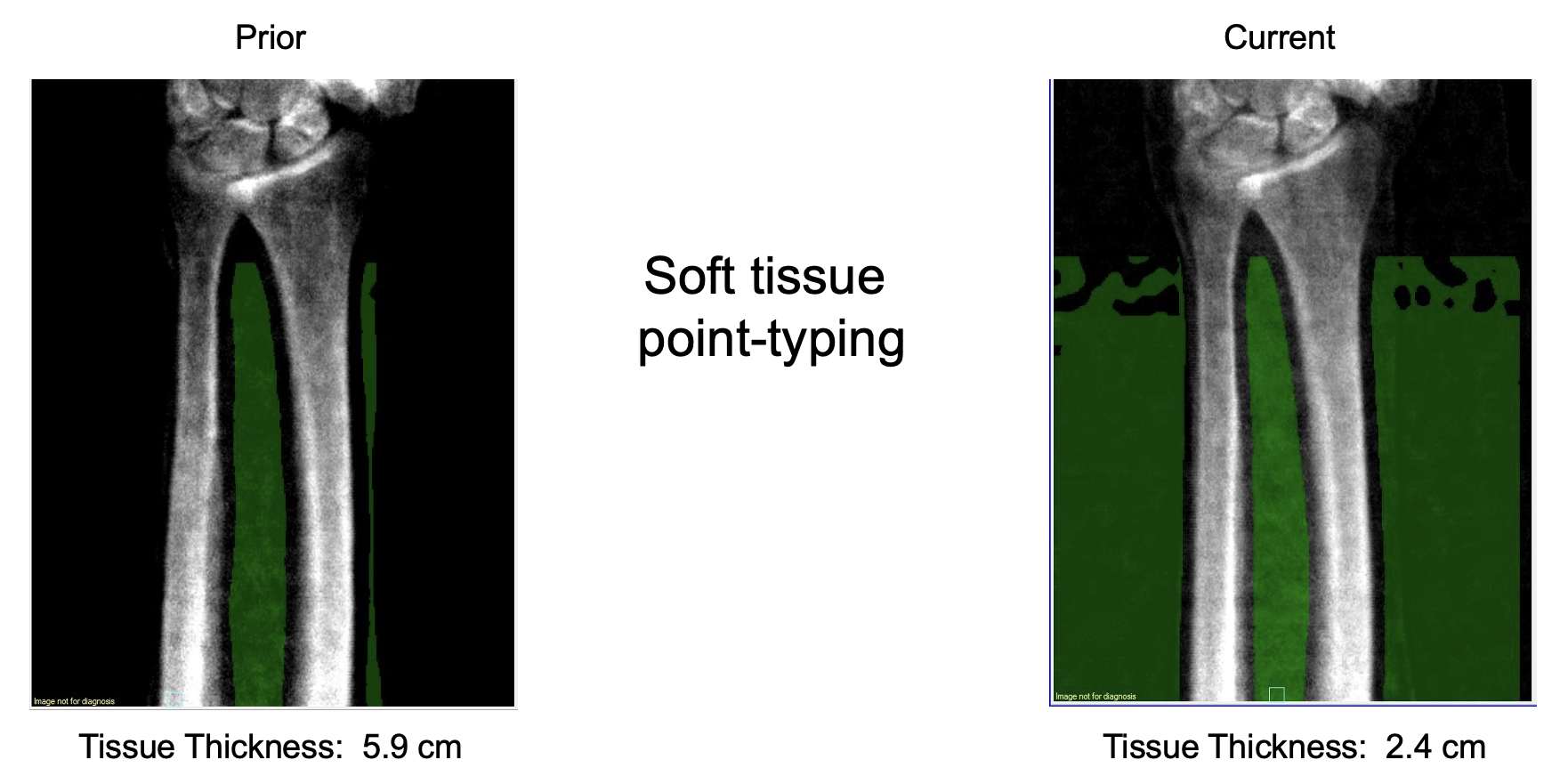
Figure 2: Current and Prior Forearm DXA (Bone view) Demonstrating BMD Increase at the .3 Radius With No Apparent Acquisition or Analysis Confounders
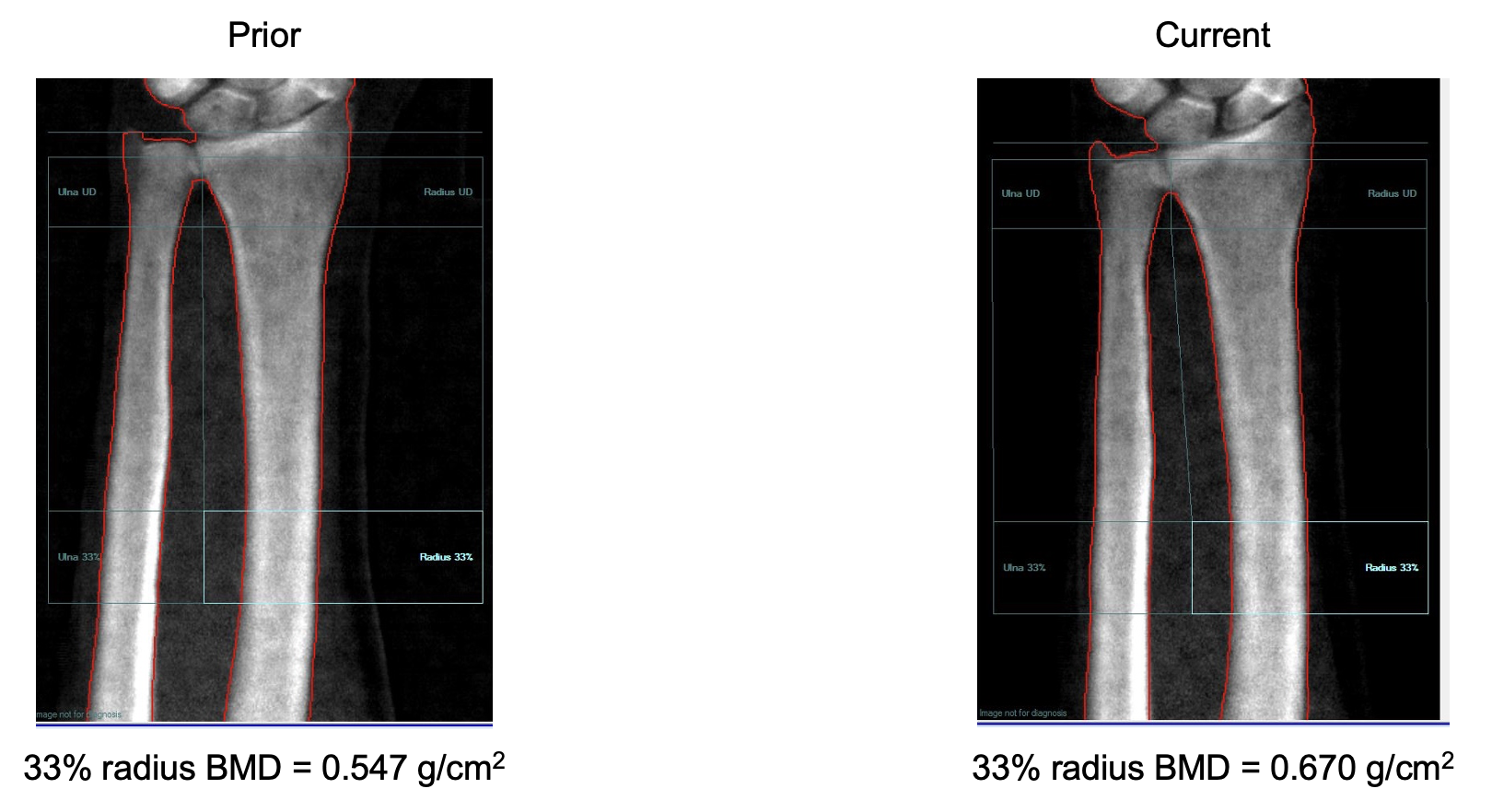
Figure 4: Forearm Image Footnotes Indicating Where Tissue Thickness Measurement is Displayed

Figure 5: Illustration of Slot on Forearm DXA Image and Forearm Positioning Board
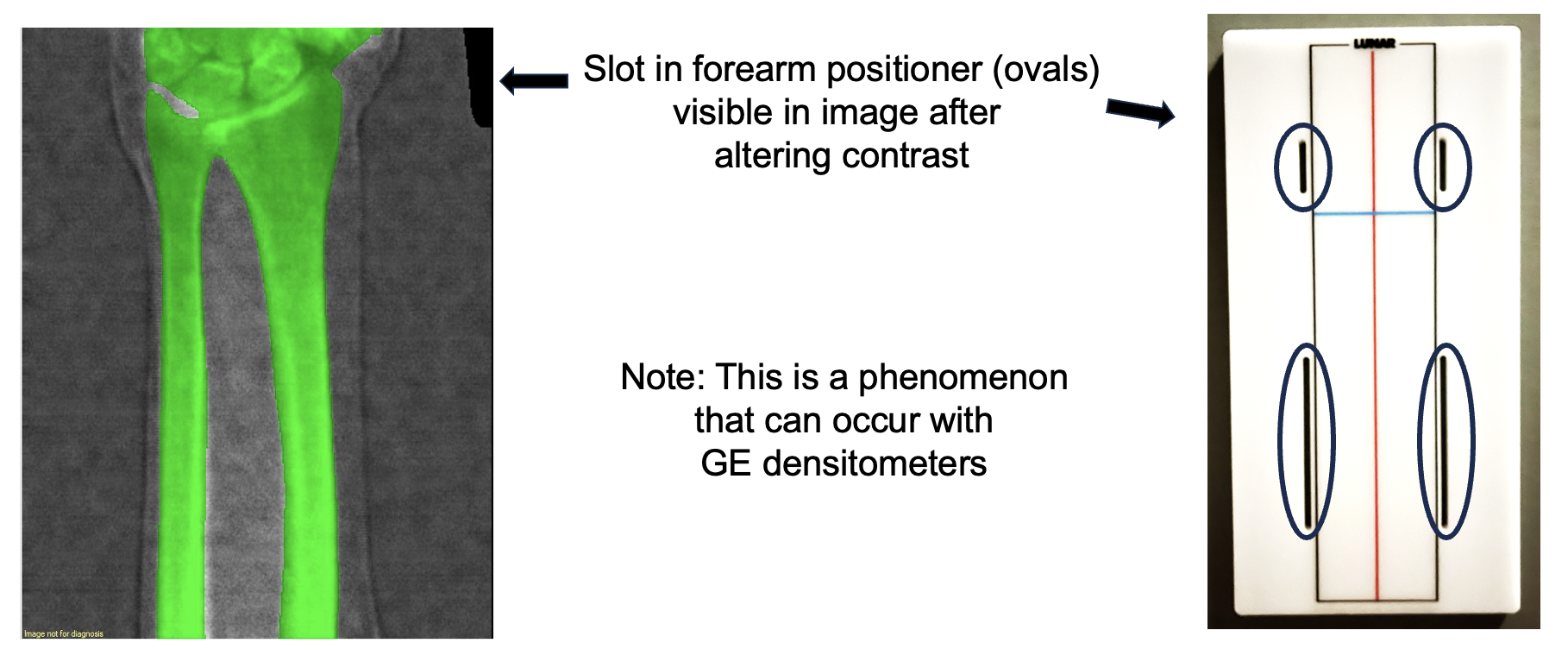
Figure 6: Adjustment of Contrast to Improve Visualization of Slot and Location of Tissue Thickness in enCORE Software (within “Information”)

79-year-old female with osteoporosis previously treated with romosozumab, followed by zoledronate 13 months prior to current DXA which was obtained to monitor treatment. BMD at the lumbar spine and mean total hip was unchanged (Image 1). Her current forearm DXA image appears normal (Image 2). However, the 33% radius BMD was 0.670 g/cm2 whereas previously it was 0.547 g/cm2 (.3 radius LSC = 0.040 g/cm2). An ~22% increase in BMD within one year seemed unlikely, particularly given no change in spine/hip BMD. As such, a technical issue was suspected. It was noted that the tissue thickness differed substantially between scans; currently being 2.4 cm vs. 5.9 cm previously. This led to assessment of the soft tissue point-typing. On the current scan the “soft tissue” includes the entire scan width, not just her forearm, thereby leading to a reduction in reported tissue thickness (Image 3). With GE densitometers, tissue thickness is noted at the bottom of report in the small print just prior to %fat (Image 4). The soft tissue point-typing error suggested the previously reported “slot-error” phenomenon (Krueger, et. al. J Clin Densitom, 2013; 16:154-159) which occurs when a slot in the forearm positioner is included in the first scan swipe (Image 5). Example of altering image contrast to visualize the slot and location of tissue thickness in GE enCORE software (Image 6).
Conclusions:
• That a “slot-error” has occurred is not apparent on the bone image utilized for reporting. Interpreters can recognize that this has occurred by a difference in tissue thickness.* *Gottinger, et. al. J Clin Densitom, 2025: in press.
• As identification of the correct soft tissue point typing is challenging at best, we recommend that the patient be re-scanned when a slot error is identified.
• With GE densitometers, DXA best-practice is for the technologist to review forearm soft tissue point-typing prior to the patient leaving.
• In this case as the technical issue was not recognized until later; no forearm BMD data were reported.
Kristyn Hare, PA-C
UW Health
Department of Orthopedics and Rehabilitation
Neil Binkley, MD
UW School of Medicine and Public Health
Division of Geriatrics