Capturing BMD of the Distal Femur and Proximal Tibia utilizing GE Orthopedic Knee Software

Acquisition Image to Capture BMD of the Distal Femur and Proximal Tibia utilizing GE Orthopedic Knee Software (Shields et al. 2005)
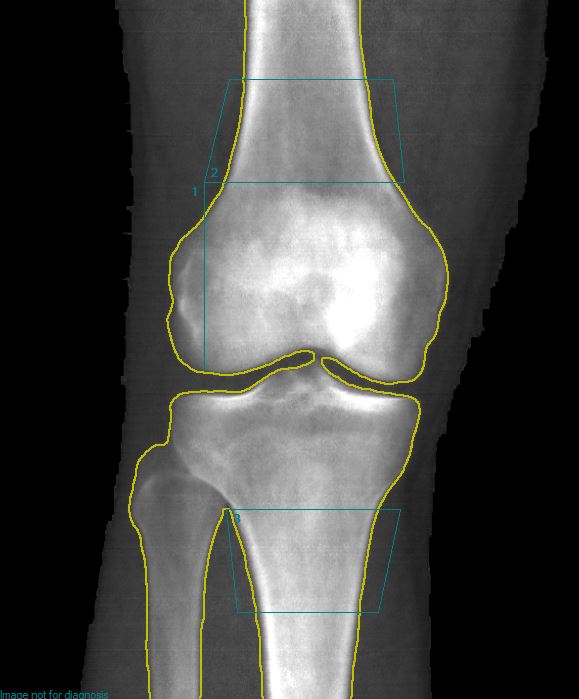
Table from Custom ROI Analysis to Capture BMD of the Distal Femur and Proximal Tibia

Knee Image from Young and Healthy Individual to Capture BMD of the Distal Femur and Proximal Tibia Utilizing GE Orthopedic Knee Software.
Acquisition and Analysis using custom ROI (Shields et al. [1]) used in several observational and randomized control trials [2-4]
Distal Femur and Proximal Tibia BMD Acquisition Protocol
Measurement procedures:
a. This scan is obtained using the GE Lunar Orthopedic knee
b. Patient positioning: Using the stabilizing triangle, secure the foot to it in a similar manner to performing the hip scan. Ensure that internal rotation is obtained to minimize the amount of overlap between the tibia and the fibula.
c. Ensure that the foam pad provided by GE is used behind the knee.
d. Ensure that lower leg is straight by adducting (not sure how to explain that it can’t be abducted) and parallel to DXA midline.
e. Identification of starting point: The starting point of the acquisition is set on the tibia approximately 4 fingers (approximately 10cm) distal from the bottom edge of the patella.
Shields et al. method to Capture aBMD at the DF and PT:
a. Measure Femur Length:
• Measure from Lateral Part of the Greater Trochanter to the lateral epicondyle. Line runs up and down the femur since it is the femur length. (Parallel to Femur). Record this length in centimeters (femur length)
b. Analyzing Knee to capture the DF and PT regions:
• Open Knee Scan
• Ensure Bone Is Marked Properly
i. Select Points
ii. Determine Whether Each of the Points of Interest (Bone, Tissue, Air, etc) are Marked Properly.
1. Image Correction: Manually correct the image point typing by identifying bone that may have been incorrectly identified. Erase the fibula bone (set to neutral) but leave what overlaps with the tibia. Identify any soft tissue surrounding the bone but user there is a neutral edge around the perimeter of the bone.
• Select ‘Results’ After All Bone is Marked Properly
• Select Analyze Tab
• Select Custom
• Choose ROI
• Line 1:
i. Select the ‘Create Line’ Option and Create a Line proximally from the Distal Edge of the Lateral Condyle up to 13% of the Femur Length
1. Length of line is calculated by multiplying the Femur Length by 0.13 (13%).
• Box 1 (Distal Femur):
i. Using the ‘Rectangle Mode’ Option, Begin Making a Box from the Most Proximal Point of Line 1 up, so that the height of the box measures 7% of the Femoral Length.
1. Height of Box is Calculated by Multiplying the Femur Length by 0.07 (7%).
2. Ensure that the Width of the Box Encompasses all of the Proximal Femur that Begins from the Proximal Point of the Femur up to the 7% Mark.
• Box 2 (Proximal Tibia):
i. Using the ‘Rectangle Mode’ Option, Begin Making a Box at the proximal edge at the uppermost point of the contact between the fibular head and the tibia.
ii. Ensure the height is 7% of the femoral length.
iii. Using the ‘Rectangle Mode’ Option, Begin Making a Box with one Corner Starting at the Uppermost Point of Contact Between the Fibular Head and the Tibia. Similarly to Box 2, Create the Box Distally from the Point of Contact 7% of the Femoral Length.
1. Height of Box is Calculated by Multiplying the Femur Length by 0.07 (7%).
2. Ensure that the Width of the Box Encompasses all of the Distal Tibia that Begins from the Tibia/Fibula Point of Contact, Distally to the 7% Mark.
3. Select “Results’ to Analyze
*Repeat Acquisition and Analysis of Other Knee as Needed
** Scan is recommended for use in persons with spinal cord injury as this is the region most susceptible to fragility fracture [5]
Christopher M. Cirnigliaro, Ph.D.
James J. Peters VA Medical Center
1. Shields RK, Schlechte J, Dudley-Javoroski S, Zwart BD, Clark SD, Grant SA et al. Bone mineral density after spinal cord injury: a reliable method for knee measurement. Arch Phys Med Rehabil. 2005;86(10):1969-73. doi:10.1016/j.apmr.2005.06.001.
2. Cirnigliaro CM, Myslinski MJ, Asselin P, Hobson JC, Specht A, La Fountaine MF et al. Progressive Sublesional Bone Loss Extends into the Second Decade After Spinal Cord Injury. J Clin Densitom. 2019;22(2):185-94. doi:10.1016/j.jocd.2018.10.006.
3. Bauman WA, Cirnigliaro CM, La Fountaine MF, Martinez L, Kirshblum SC, Spungen AM. Zoledronic acid administration failed to prevent bone loss at the knee in persons with acute spinal cord injury: an observational cohort study. J Bone Miner Metab. 2015;33(4):410-21. doi:10.1007/s00774-014-0602-x.
4. Oleson CV, Marino RJ, Formal CS, Modlesky CM, Leiby BE. The effect of zoledronic acid on attenuation of bone loss at the hip and knee following acute traumatic spinal cord injury: a randomized-controlled study. Spinal Cord. 2020. doi:10.1038/s41393-020-0431-9.
5. Morse LR, Biering-Soerensen F, Carbone LD, Cervinka T, Cirnigliaro CM, Johnston TE et al. Bone Mineral Density Testing in Spinal Cord Injury: 2019 ISCD Official Position. J Clin Densitom. 2019;22(4):554-66. doi:10.1016/j.jocd.2019.07.012.